





Complete this Autopac Accident Report as soon as possible after the accident. Use it to help you make your Autopac Report.
Time: __________________ Date: ________________
Weather: __________________________________________________________
Light: _____________________________________________________________
(dark, dust, dawn, day)
Note: The Highway Traffic Act requires the driver of the vehicle
involved in an accident, to give written information to anyone that was
injured or whose property was damaged
OTHER DRIVER
Name: ____________________________________________________________
Address: __________________________________________________________
Telephone: ________________________________________________________
Driver's License #: __________________________________________________
Vehicle: ___________________________________________________________
(year, make, model, body type, hatchback)
License Plate #: ____________________________________________________
Vehicle Owner's Name: _______________________________________________
Insurance Company: _________________________________________________
Policy #: ___________________________________________________________
Insurance Agent: _____________________________________________________
Address: ___________________________________________________________
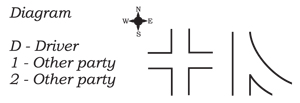
THE ACCIDENT
What happened? _____________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
What injuries did people have? __________________________________________
___________________________________________________________________
___________________________________________________________________
WITNESSES
Name: ______________________________________________________________
Address: ___________________________________________________________
Telephone: _________________________________________________________
Name: ______________________________________________________________
Address: ___________________________________________________________
Telephone: _________________________________________________________
Call Police when:
PLUS we offer direct billing to MPI!
‹ Return from Autopac Accident Report to Auto Body Repair Winnipeg









 |
| 